







Systemic medications can have significant and potentially visually debilitating effects on the retina. Certain medications, such as hydroxychloroquine (HCQ) and pentosan polysulfate (PPS), can cause irreversible vision loss if not monitored carefully for ocular toxicity and stopped at the earliest signs of toxicity.1 Corticosteroids in any form can cause central serous retinopathy.2 Systemic medications used to treat cancer, seizures, heart disease, and other conditions can have varied effects on the retina, ranging from benign crystalline retinal deposits to transient dyschromatopsia to subretinal fluid.
Once retinal toxicity occurs, visual impairment is irreversible in many cases,1 so familiarity with screening guidelines is essential to prevent vision loss. No gold standard currently exists for identifying ocular toxicity prior to its development, necessitating a multipronged approach to screening for toxicity.
This is the first article in a 2-part series on the retinal complications of systemic drug therapy. This first installment will focus on HCQ and PPS; part 2, which will appear in the October 2023 issue of New Retinal Physician, will examine other medicines that can cause retinal toxicity, including chemotherapeutic agents and other cancer-fighting medicines, antiseizure and antipsychotic medications, heart medications, and antivirals used to treat human immunodeficiency virus (HIV).

FIGURE 1: Long-term use of hydroxychloroquine sulfate can result in retinal toxicity. High-risk factors include use of the medication for more than 5 years, or a total cumulative dose of more than 1000 g.
IMAGE COURTESY STOCK.ADOBE.COM / MBRUXELLE
HYDROXYCHLOROQUINE
Chloroquine (Aralen; Sanofi) is used as an antimalarial and antiamoebic drug, especially in developing countries. Hydroxychloroquine (Plaquenil; Sanofi) is a less toxic derivative of chloroquine. It is used in the United States to treat rheumatological conditions, such as lupus or rheumatoid arthritis. HCQ gained notoriety during the SARS CoV-2 pandemic as a potential treatment for COVID-19, although studies ultimately indicated the drug was unlikely to be effective in treating the coronavirus.
Hydroxychloroquine is a known retinal toxin. The recommended daily dose of HCQ, based on guidelines from the American Academy of Ophthalmology (AAO) Preferred Practice Patterns (2016), is less than 5 mg per kg of real body weight per day, which has been shown to correlate better with maculopathy risk compared to the ideal weight. No similar demographic data are available for chloroquine, but older literature suggests less than 2.3 mg/kg real weight.3 At these recommended doses, the risk of toxicity is less than 1% up to 5 years and less than 2% up to 10 years; however, after 20 years the risk of toxicity increases sharply to almost 20%. Major risk factors for toxicity include high doses, long duration, concomitant renal disease, concomitant macular/retinal disease, and/or use of tamoxifen.3

FIGURE 2: Imaging of the left (A) and right (B) eyes of a 29-year-old woman who had been treated with a daily dose of 400 mg of hydroxychloroquine for 14 years—a cumulative dose of exceeding 2000 g. Spectral domain optical coherence tomography (SD-OCT) demonstrates perifoveal thinning of the ellipsoid layer and outer retina, with a preserved central fovea (the “flying saucer” sign of advanced toxicity; see also Figure 4). Fundus autofluorescence (FAF) imaging demonstrates perifoveal hyperautofluorescence, surrounded by granular hyperautofluorescence/hypoautofluorescence.
IMAGES COURTESY HADAS NEWMAN, MD, AND SHIRI SHULMAN, MD
The AAO’s screening guidelines for chloroquine and hydroxychloroquine retinopathy include a baseline fundus exam to rule out pre-existing maculopathy, fundus autofluorescence (FAF) imaging, automated Humphrey visual fields (HVF) 10-2 testing, and spectral domain optical coherence tomography (SD-OCT) imaging. Annual screening should commence after 5 years for patients on acceptable doses and without major risk factors.3
Asian patients, however, often show an extramacular pattern of damage, which should be considered during evaluation. Visual field testing (eg, HVF 24-2 or 30-2) and peripheral SD-OCT imaging should encompass the extramacular area.3,4 Fundus autofluorescence is especially helpful in such cases. Multifocal electroretinogram (mf-ERG) can be a useful tool if available in equivocal cases, although this testing may be difficult to obtain outside of academic institutions.5
The following screening tests are no longer recommended due to inadequate sensitivity: fundus photography, time-domain optical coherence tomography, fluorescein angiography, full-field electroretinography, Amsler grid, color vision testing, and electrooculography.2
SIGNS OF HYDROXYCHLOROQUINE TOXICITY
On fundus autofluorescence, early maculopathy presents as a pericentral ring of increased FAF intensity, appearing as a hyperfluorescent glow. This may be seen in hydroxychloroquine toxicity before retinal pigment epithelium (RPE) degeneration develops and noted on fundus photographs or dilated eye examination. This represents early photoreceptor damage from accumulation of outer segment debris.3 The classic “bullseye” maculopathy appearance is noted in advanced stages. A pericentral ring of mottled or dark area of hypoautofluorescence denotes RPE loss and atrophy.3
In visual field testing, central field abnormalities—most frequently in the inferotemporal region—correspond to superonasal field defects on HVF 10-2.5
Early toxicity can demonstrate a normal appearance on SD-OCT or appear as subtle irregularities of the ellipsoid zone.6 This progresses to localized thinning/disruption of the photoreceptor layers in the parafoveal region. Later findings include progressive disruption of the peri-foveal ellipsoid zone with sparing of the foveal photoreceptors, leading to the characteristic “flying saucer sign.” Undiagnosed maculopathy will eventually lead to the disruption of both the parafoveal and foveal photoreceptors and RPE.5,6
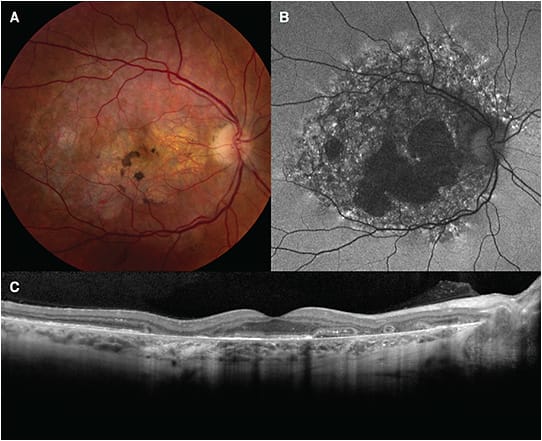
FIGURE 3. Fundus imaging of a patient with moderately advanced atrophic disease in the setting of chronic PPS exposure. Color fundus photography of the right eye demonstrates prominent paracentral atrophy of the retinal pigment epithelium surrounded by subtle pale yellow deposits (A). Fundus autofluorescence imaging demonstrates a well-defined region in the posterior pole with densely packed hyperautofluorescent and hypoautofluorescent spots. There is hypoautofluorescence associated with retinal pigment epithelium atrophy encroaching on the foveal center (B). Optical coherence tomography imaging demonstrates paracentral atrophy with outer retinal tubulations (C).
IMAGES COURTESY RACHEL SHAH, MD, AND NIERAJ JAIN, MD
The multifocal ERG is the most sensitive tool for detecting localized, subtle central retinal defects secondary to early stages of toxicity. Paracentral amplitude loss occurs due to decreased retinal function in the susceptible perifovea. Disadvantages of this modality are lack of ready accessibility, dependence on patient cooperation, specialized staff training for administration and interpretation, and overall cost.7
Hydroxychloroquine use must be stopped once early signs of maculopathy are suspected or detected. Stopping the medication does not always prevent retinopathy progression and can continue for years after medication cessation. The risk of progression after medication cessation correlates to the level of toxicity at the time the medication is stopped.6 The risk is low if minimal to no toxicity is present and higher if bullseye maculopathy or reduction in central foveal thickness are present. Patient can be advised of risk of further vision loss after medication cessation depending on the level of retinopathy. The decision to stop the medication needs to be made in conjunction with the patient and their managing physician to ensure medical risks such as rheumatologic flares are managed accordingly.
PENTOSAN POLYSULFATE
Pentosan polysulfate is the only FDA-approved drug (Elmiron; Janssen Pharmaceuticals) for bladder discomfort due to interstitial cystitis. Long-term use, with a median time of exposure 14 years, can cause pigmentary maculopathy.8 This can mimic age-related macular degeneration (AMD) or pattern dystrophy.8,9 The most common symptoms are blurred or decreased vision (66%) and nyctalopia (32%).9
Paracentral pigment clumps amid a background of yellow subretinal deposits are noted on fundus examination.9 Vitelliform deposits and patchy paracentral RPE atrophy, similar in appearance to pattern dystrophy, can also be present.10 Fundus autofluorescence demonstrates dense hyperfluorescent and hypoautofluorescent spots that involve the fovea. The speckled hyperfluorescent spots correspond to vitelliform deposits that can extend to the peripapillary region.9,10 SD-OCT demonstrates irregularity to the outer retinal bands with a focal thickening of the RPE. Advanced PPS maculopathy demonstrates RPE atrophy with outer retinal thinning.9,10
A high index of suspicion for PPS maculopathy should be present in patients with “atypical” AMD or pattern dystrophy or younger patients (in their 40s or 50s) with AMD. Check these patient’s medication lists.
Patients started on a long-term course of PPS should undergo a dilated fundus baseline exam, color fundus photography, FAF imaging, and OCT imaging of the macula. Patients with underlying macular disease should be started on PPS cautiously and screened closely. Once they start the drug, repeat screening with the same fundus imaging/evaluation should be done annually.9,10 The risk of toxicity increases significantly in patients exposed to doses greater than 1500 g.11
In the event of toxicity, discuss drug discontinuation with the patient’s urologist. Caution the patient and urologist that effects on the eye can continue even after the drug is stopped. These guidelines will change as more information on the condition is known.9
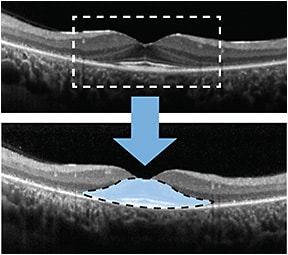
FIGURE 4. Thinning of the perifoveal photoreceptor inner segment/outer segment junction with preservation of outer retinal structures in the central fovea creates the “flying saucer” sign characteritic of retinal toxicity.
IMAGE COURTESY HADAS NEWMAN, MD, AND SHIRI SHULMAN, MD
CONCLUSION
Management of patients who are taking HCQ or PPS requires awareness and concern for the potentially serious underlying issue of retinal toxicity. Patients’ medication usage history must be carefully reviewed and monitored, because once retinal damage has occurred it is generally irreversible. NRP
REFERENCES
- Tehrani R, Ostrowski RA, Hariman R, Jay WM. Ocular toxicity of hydroxychloroquine. Semin Ophthalmol. 2008;23(3):201-209. doi:10.1080/08820530802049962
- Daruich A, Matet A, Dirani A, et al. Central serous chorioretinopathy: recent findings and new physiopathology hypothesis. Prog Retin Eye Res. 2015;48:82-118. doi:10.1016/j.preteyeres.2015.05.003
- Marmor MF, Kellner U, Lai TY, Melles RB, Mieler WF; American Academy of Ophthalmology. Recommendations on screening for chloroquine and hydroxychloroquine retinopathy (2016 revision). Ophthalmology. 2016;123(6):1386-1394. doi:10.1016/j.ophtha.2016.01.058
- Melles RB, Marmor MF. Pericentral retinopathy and racial differences in hydroxychloroquine toxicity. Ophthalmology. 2015;122(1):110-116. doi:10.1016/j.ophtha.2014.07.018
- Rahimy E, Vander J. Multimodal imaging in Plaquenil toxicity. Review of Ophthalmology. August 6, 2014. Accessed May 9, 2023. https://www.reviewofophthalmology.com/article/multimodal-imaging-in-plaquenil-toxicity
- Lally DR, Heier JS, Baumal C, et al. Expanded spectral domain-OCT findings in the early detection of hydroxychloroquine retinopathy and changes following drug cessation. Int J Retina Vitreous. 2016;2:18. doi:10.1186/s40942-016-0042-y
- Tsang AC, Ahmadi Pirshahid S, Virgili G, Gottlieb CC, Hamilton J, Coupland SG. Hydroxychloroquine and chloroquine retinopathy: a systematic review evaluating the multifocal electroretinogram as a screening test. Ophthalmology. 2015;122(6):1239-1251.e4. doi:10.1016/j.ophtha.2015.02.011
- Pearce WA, Chen R, Jain N. Pigmentary maculopathy associated with chronic exposure to pentosan polysulfate sodium. Ophthalmology. 2018;125(11):1793-1802. doi:10.1016/j.ophtha.2018.04.026
- Stuart A. Pentosan polysulfate maculopathy: an elusive masquerader. EyeNet Magazine. 2020;24(3): 28-30. https://www.aao.org/eyenet/article/pentosan-polysulfate-maculopathy
- Shah VA, Tripahy K, Zhu I, Hsu J, Lim JI, Chhablani J. Drug-induced maculopathy. EyeWiki.aao.org . November 6, 2022. Accessed May 9, 2023. https://eyewiki.aao.org/Drug_induced_maculopathy
- Hadad A, Helmy O, Leeman S, Schaal S. A novel multimethod image analysis to quantify pentosan polysulfate sodium retinal toxicity. Ophthalmology. 2020;127(3):429-431. doi:10.1016/j.ophtha.2019.10.013