







When patients present with intraocular inflammation, the differential diagnosis and workup can prove to be a challenging task. This can be especially daunting for ophthalmologists in training as well as those who are not used to treating intraocular inflammation on a regular basis.
When approaching intraocular inflammation, the guiding principle is to first rule out an infection through clinical, serologic, or specimen analysis. Once an infectious process is ruled out, steroid treatment is in order in most cases. This approach might be reductionist, but it aims to be efficient in obtaining the necessary data without overburdening the patient or the medical system.
Theory often oversimplifies the nuances of clinical practice, however, and in this process trainees and general ophthalmologist can be prone to overordering tests. An extensive workup is often unnecessary and in fact can be detrimental to the process of narrowing a proper diagnosis. More importantly, ordering unnecessary tests can lead to excessive costs and increased physical discomfort for the patient. According to one study conducted at the New York Eye and Ear Infirmary, the cumulative average cost of services for patients with anterior uveitis was $415, while the expenditure on panuveitis patients averaged $791 for their workup alone.1
Given our personal experience at a tertiary referral center, we have seen residents order unnecessary tests in the emergency room while assessing uveitis patients and have received referrals that do not address the underlying process clearly. As an example, we have seen young patients with anterior uveitis tested for HLA-A29 and HLA-B51 without any clinical basis. Another common pitfall is testing for serum levels of angiotensin-converting enzyme (ACE) and lysozyme routinely on patients without a proper knowledge of the pretest probability.
A different instance is the well-intended, but often fraught, manner of working up patients for ocular syphilis. The incidence of ocular syphilis is on the rise, with approximately 55,400 people newly infected each year in the United States.2 In the age of pre-exposure prophylaxis, the numbers are expected to increase. In 2018, it was estimated that men accounted for approximately 86% of all cases of syphilis in the United States.3
Ocular syphilis is an entity that the ophthalmologist should always consider and work up appropriately. However, for an alarming number of patients, nontreponemal tests are ordered as an initial workup. This delays the appropriate course of action and treatment until a proper treponemal test is obtained.
NEW MOBILE APP
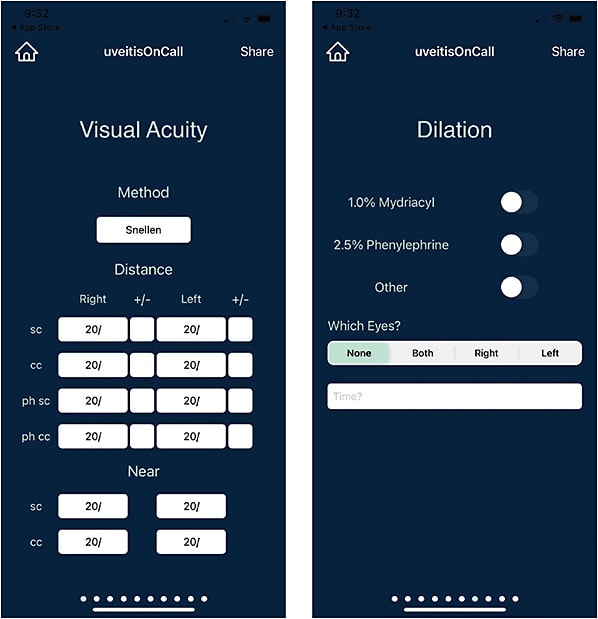
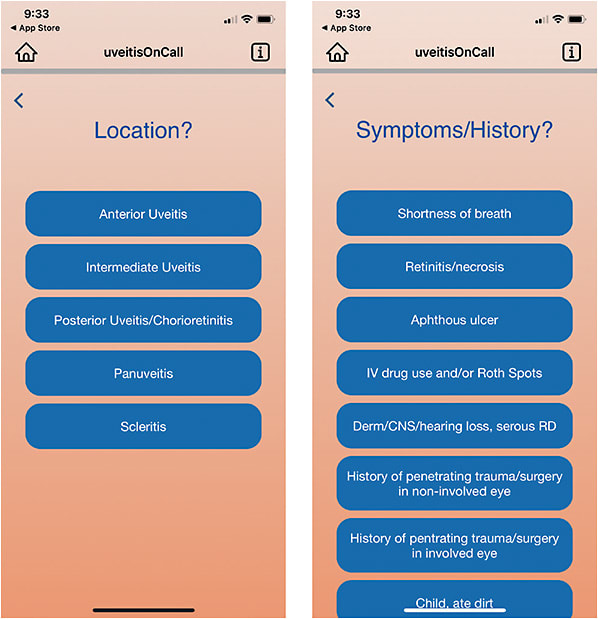
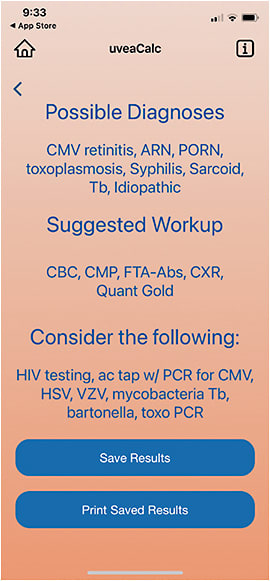
UveitisOnCall, a new mobile phone application created in partnership with mHealth Wellness (https://www.mhealthwellness.com ), provides an alternative way for medical providers to evaluate signs and symptoms of uveitis, using an evidence-based algorithm to work through numerous possible diagnoses. When patients present with uveitis, the doctor can input eye exam findings, as well as the location of the inflammation, into the user-friendly uveitisOnCall interface, and quickly arrive at a suggested workup and differential diagnosis.
To test the app, we conducted a prospective study of 25 patients presenting with uveitis and compared the workup and differential ordered by the on-call resident, the suggested results based on the app, and the workup and differential ordered by an attending retinal specialist. Our inclusion criteria were patients of all ages presenting with anterior uveitis, intermediate uveitis, posterior uveitis, chorioretinitis, panuveitis, or scleritis with no prior known diagnosis.
We then calculated the concurrence of the application with the retina specialist. We also compared the testing ordered by the resident to the app’s recommendaton. We found that in 84% of the cases, the app and the retina specialist agreed on the same initial laboratory workup as well as the top 3 differential diagnoses.
CONCLUSION
There is no substitute for a thoughtful and thorough ocular examination, but the uveitisOnCall mobile app can be a great tool for ophthalmology residents, comprehensive ophthalmologists, and other allied health care providers to guide the workup for patients presenting with uveitis. The application aims to cast a diagnostic net in which potentially visually devastating diseases are evaluated and accounted for. We believe that it can help reduce the healthcare costs associated with unnecessary testing while expediting the process by which laboratory workup and care for the uveitis patient is given. The application should be used with a framework as to how to approach ocular inflammation in a systematic manner. NRP
Editor’s note: The uveitisOnCall app is designed to work with Apple iOS devices and is available for download from the App Store.
REFERENCES
- Lee OL, Tari SR, Samson CM. Cost-analysis of uveitis patient visits at the New York Eye and Ear Infirmary. Invest Ophthalmol Vis Sci. 2007;48(13):2406.
- Koundanya VV, Tripathy K. Syphilis ocular manifestations. In: StatPearls. Treasure Island (FL): StatPearls Publishing; February 21, 2022.
- Oliver SE, Aubin M, Atwell L, et al. Ocular syphilis—eight jurisdictions, United States, 2014-2015. MMWR Morb Mortal Wkly Rep. 2016;65(43):1185-1188. doi:10.15585/mmwr.mm6543a2