







Diabetic macular edema (DME) is the most frequent cause of visual loss in patients with diabetic retinopathy (DR). It may occur at any stage of DR; however, it is more common and more severe in the later stages. As the number of patients with diabetes continues to grow, the prevalence of DME is proportionally increasing. Of the more than 30 million people in the United States who have diabetes, approximately 25% develop DR, and an estimated 10% are affected by DME.1
Here, I highlight some important points in clinical practice that can help in better diagnosing DME and guide you to the most effective line of treatment.
FUNDUS FLUORESCEIN ANGIOGRAPHY
Does fundus fluorescein angiography (FFA) still have a role in DR and DME management, or can you just treat based on optical coherence tomography (OCT) and clinical correlation alone? Some physicians consider baseline FFA necessary. Sometimes it might be difficult to obtain an angiogram, especially with renal patients on dialysis (fluorescein dye itself is not toxic but can cause staining of skin and conjunctiva, so you might consider it if the patient is due on dialysis). Also, it can be challenging to use the dye in asthmatic and allergic patients who might develop severe or life-threatening reactions to it.
Sometimes, we need to use oral fluorescein in children (usually mixed in orange juice as it has a bitter taste).
In Egypt, where I started my retina practice, we used to have limited resources, including access to fluorescein ampoules. To overcome this, a half-dose of the fluorescein ampoule is used for one patient (considering the patient weight). A few times we could not detect any dye in the eye (even after a bolus 5 ccs dose of 10% NaFl). We discovered that the dye might circulate in the aortic arch without getting into the carotid. In such a case, we used to wait 10 to 15 minutes, and if nothing changes, we’d repeat the full dose the same day.
Fundus fluorescein angiography has always been considered in clinical practice for two reasons that might be difficult to obtain with any other imaging modality: ischemia and leakage.
• FFA and Ischemia. Although innovative imaging modalities are now available to obtain a wider view of the retina, dye angiography has the widest available view. The extent of peripheral ischemia varies and fluctuates over time, changes dynamically in response to treatment, and correlates with the severity of edema and vision loss. This can be used to monitor and even predict response to different treatments.2
Widefield image mapping of the peripheral ischemia in patients with rebound edema can guide treatment with guided/targeted laser photocoagulation, especially if you plan to treat your patient with macular photocoagulation as well.3
• FFA and Leakage. Some researchers suggest that fluorescein angiographic-guided laser treatment of DME may be superior to treatment that does not involve the use of fluorescein angiography (FA). The treatable lesions on FA are leaking microaneurysms, areas of diffuse leakage, and areas of non-perfusion in the macula. You might consider fluorescein angiogram at presentation before treating DME, as it facilitates the decision-making process as which initial treatment could be.4
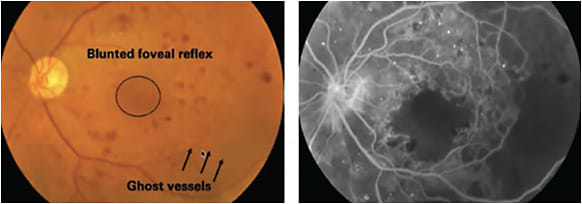
Although it can be identified clinically, ischemic maculopathy-associated DME (blunt foveal reflex with ghost vessels, Figure 1) can be difficult to quantify clinically, and you need FFA for this purpose. Focal laser (prompt vs. rescue) can be then considered based on the clinical scenario. Focal circinate lesions that are leaking on FFA can also be targeted using focal laser. It is important to consider that an ischemic macula leads to a massive release of VEGF, which might worsen DME and causes its recurrence.
Also at the same time, an ischemic thin area usually gets atrophied over time and it can be risky to do focal laser over it. Intraretinal microvascular abnormalities (IRMAs) are shunt vessels and appear as abnormal branching or dilation of existing blood vessels (capillaries) within the retina that act to supply areas of non-perfusion in diabetic retinopathy. These vessels represent either new vessel growth within the retina or remodeling of pre-existing vessels through endothelial cell proliferation stimulated by hypoxia bordering areas of capillary nonperfusion.
IRMA is one of the defining features of severe non-proliferative diabetic retinopathy. When compared with neovascularization (NV) in proliferative disease, IRMAs are slightly larger in caliber with a broader arrangement and are always contained to the intraretinal layers. Conversely, NV tends to be much finer and delicate in caliber and is sometimes more focal in location depending on its severity. Although they can be delineated clinically, FA can help to differentiate it from NV, which often shows late leakage, whereas IRMAs traditionally do not leak. IRMAs have a high risk of progression to NV and proliferative diabetic retinopathy (PDR).
WELCOME OCT-A
OCT angiography (OCT-A) is one of the newest diagnostic technologies available to retina specialists, and it is expected to be valuable in the management of DME. For example, OCT-A can detect lesions relevant to DME, such as microaneurysms.5
It is important to note that we cannot rely on OCT-A alone in cases in which part of the plan is to treat with focal laser.
First, not all microaneurysms are visible, only a subset. There is an indication that the more hyporeflective microaneurysms visible on structural OCT are less likely to be detected on OCT-A. Second, OCT-A does not discern which microaneurysms are leaking. Therefore, it does not indicate which ones to treat.
OCT-A can be a potent and useful tool for evaluating macular ischemia, and is quite relevant given what we know about disorganization of retinal inner layers (DRIL), which leads us to suspect it. OCT-A has shown us that ischemia may involve different retinal layers. Following its extent may be useful from a prognostic standpoint.6
Finally, OCT-A appears to be much more sensitive than fluorescein angiography for assessing macular perfusion. This is likely to be extremely helpful as we collectively continue to monitor what impact anti-VEGF therapy may or may not have on macular perfusion.7
OCT’S ROLE IN DIAGNOSING DME
The extent to which OCT has transformed how retina specialists diagnose and manage diabetic eye disease is impressive (Figure 4). OCT is now the gold standard for diagnosing DME, monitoring treatment response, and determining when to retreat. The question is whether OCT is always required on initial presentation with 20/20 vision to assist in classifying eyes as center or non-center involved DME, or if differentiation on a clinical exam is sufficient.

It is important to quantitate the amount of edema present and, in cases initially sparing the fovea, determine whether there’s encroachment toward the center over time. This information will help measure the patient’s progress and assist you in making treatment decisions.
Volume scans may provide as much information as you need to determine treatment algorithms and strategy and do so rapidly. In a busy practice, the best evidence to date indicates that looking at a volume scan with particular emphasis on the central subfield is adequate to treat most patients. When spectral-domain OCT is used, it may be advisable to order a macular cube scan to determine the thickness in the nine macular subfields (as defined by the standard ETDRS grid) so the patient can be followed longitudinally and change detected.
Some clinicians may order a higher-resolution raster scan as well to check whether there are any vitreomacular interface abnormalities, which could affect patient management. You may choose to scroll through a patient’s B scans yourself, knowing that it can take just seconds and feeling that you would like to view the automated placement of the inner and outer retinal boundary lines to decide whether the information on the map should be accepted, rather than taking it at face value.
In current times, in patients who have reduced vision but no significant edema, color photographs and angiography at baseline might be able to identify features suggestive of macular ischemia.
Once we decided to treat, we use OCT to monitor the response. Following DRCR.net Retinal Network site and other trial protocols, our focus is normalizing central retinal thickness on OCT to the greatest extent possible. When that is achieved, we continue to use OCT to watch for recurrence and determine the best interval between treatments.8
OCT potentially has a role in DME management beyond the assessment of retinal thickness. It identifies other retinal abnormalities that may help inform our expectations of treatment outcomes and patient prognosis. Several potential biomarkers can be assessed. Disorganization of the retinal inner layers (DRIL), for example, seems to be a sign that ischemia is likely present and visual outcomes may not be as good.9
OCT also shows the integrity of the outer retinal bands, i.e., the ellipsoid zone and external limiting membrane. Solid data that have been published indicate that eyes with disrupted outer retinal bands may have inferior vision recovery after treatment.
Hyperreflective spots are another OCT-visualized biomarker being evaluated for prognostic value. Commonly, these spots or dots are evidence of lipid exudates. When we see a significant number of such exudates, especially if they are tracking toward the foveal center, we increasingly interpret it as a negative prognostic sign. Furthermore, hyperreflective spots are a reminder to make sure the patient is working with his/her internist on lipid level control. It has also been theorized that even very small hyperreflective spots may be significant, possibly indicating activated microglia or migrating RPE cells, and/or markers of inflammation.10
Larger prospective trials will determine just how closely DRIL, disruption of the outer retinal bands, and hyperreflective spots are associated with poorer visual outcomes and less-than-desired response to anti-VEGF therapy and how we should use the findings in day-to-day practice. Other OCT biomarkers, such as diffuse vs. focal/cystoid DME and the presence of subretinal fluid, were previously thought to be relevant to how an eye would respond to therapy. However, they have not proved to be important in terms of anti-VEGF therapy or how patients should be managed.
To sum up, OCT helps you classify and monitor response to treatment and helps to discuss the prognosis with the patient before even proceeding with the initial management. Sometimes, a huge DME can disappear after treatment while the vision remains the same due to either DRIL or outer retinal atrophy.
CONCLUSION
Diabetic macular edema represents a significant public health challenge. Many patients are undiagnosed and untreated, and even those treated with standard therapy may respond poorly and progressively lose vision.
Insight into the pathophysiology of DME guided by the proper diagnostic imaging modality can help you move on with the next step and it has also led to novel treatments, including anti-VEGF and corticosteroid-based treatment strategies. NRP
REFERENCES:
- Tripathy K, Sharma YR, Karthikeya R, et al. Recent advances in management of diabetic macular edema. Curr Diabetes Rev. 2015;11(2):79-97.
- Schachat AP. A new approach to the management of diabetic macular edema. Ophthalmology. 2010;117(6):1059-1060.
- Wessel MM, Nair N, Aaker GD, Ehrlich JR, D’Amico DJ, Kiss S. Peripheral retinal ischaemia, as evaluated by ultra-widefield fluorescein angiography, is associated with diabetic macular oedema. Br J Ophthalmol. 2012;96(5):694-698.
- Najeeb BH, Simader C, Deak G, et al. The distribution of leakage on fluorescein angiography in diabetic macular edema: a new approach to its etiology. Invest. Ophthalmol. Vis. Sci. 2017;58(10):3986-3990.
- Hwang TS, Jia Y, Gao SS, et al. Optical coherence tomography angiography features of diabetic retinopathy. Retina 2015;35:2371.
- Hwang TS, Gao SS, Liu L, et al. Automated quantification of capillary nonperfusion using optical coherence tomography angiography in diabetic retinopathy. JAMA Ophthalmology 2016;134:367-373.
- Soares M, Neves C, Marques IP, et al. Comparison of diabetic retinopathy classification using fluorescein angiography and optical coherence tomography angiography. Br J Ophthalmol. 2017 Jan;101(1):62-68.
- Couturier A, Rey PA, Erginay A, et al. Widefield OCT-angiography and fluorescein angiography assessments of nonperfusion in diabetic retinopathy and edema treated with anti-vascular endothelial growth factor. Ophthalmology 2019;126(12):1685-1694.
- Ehlers JP, Uchida A, Hu M, Figueiredo N, Kaiser PK, Heier JS. Higher-Order Assessment of OCT in Diabetic Macular Edema from the VISTA Study: Ellipsoid Zone Dynamics and the Retinal Fluid Index, Ophthalmology Retina 2019;3(12):1056-1066.
- Vujosevic S, Bini S, Torresin T, Berton M, Midena G, Parrozzani R. Hyperreflective retinal spots in normal and diabetic eyes: B-scan and en face spectral domain optical coherence tomography evaluation. Retina. 2017; 37(6):1092-1103.