







For the past several decades, there have been a number of reasonable options when deciding how to treat a primary rhegmatogenous retinal detachment (RRD). Choices range from pars plana vitrectomy (PPV), to pneumatic retinopexy (PnR), to scleral buckle (SB), and, finally, to combined pars plana vitrectomy-scleral buckle (PPV-SB). All techniques have been considered reasonable options for routine cases, and depending where a patient goes for treatment, they will be offered different choices. In the absence of a clear favorite, in most situations, the surgeon chooses the treatment that he or she wants to perform.
There are many factors that could potentially influence this decision, including patient characteristics (e.g., chronicity); location of the break(s); other pathology, such as lattice degeneration and presence of a posterior vitreous detachment; surgeon characteristics, such as age, training, experience, and how busy their practice is; and system factors, such as access to the operating room, renumeration, and ease of follow-up. The surgeon considers all of these factors before deciding on a treatment. This has been the approach to date because all surgical techniques have been generally considered reasonable on the basis of achieving retinal reattachment and decent functional outcomes.
SURGICAL TECHNIQUES’ IMPACT ON INTEGRITY
A new era in retinal detachment repair is now upon us, inspired by the recent advances in multimodal imaging and increasing evidence from randomized trials. The PIVOT trial1 recently demonstrated that patients undergoing PnR had superior ETDRS visual acuity, less vertical metamorphopsia, improved vision-related quality of life in the first 6 months, and less morbidity with a less-invasive procedure in PnR compared with PPV.
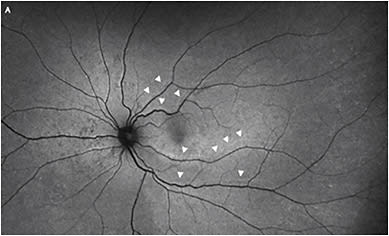
There is also emerging evidence that the integrity of retinal reattachment varies with the surgical technique chosen. A recent study demonstrated that PnR was associated with a greater chance of achieving a high integrity retinal attachment (HIRA) compared with PPV.2 This may be related to several factors, but particularly that PnR is an RPE pump-based procedure where the gas bubble occludes the retinal break and the RPE pump is responsible for slowly achieving retinal reattachment. Furthermore, PnR utilizes a smaller gas bubble, which applies less buoyant force to a smaller area of retina, thereby increasing the chance of HIRA. To the contrary, PPV is associated with a rapid iatrogenic process of retinal reattachment in which fluid is manually removed from the subretinal space over a short period of time. Moreover, large gas fills are used with a large buoyant force applied to a large area of retina, which likely leads to a high risk of retinal displacement or a low integrity retinal attachment (LIRA) (Figure 1).
KEEPING INTEGRITY AT THE FOREFRONT
No longer is it reasonable to choose primarily based on physician factors. One must keep functional outcomes from randomized trials and the concept of integrity at the forefront of the decision-making process. The days of single-operation reattachment rate being the only main outcome of interest are numbered, and the emphasis will shift from “How often will a retinal reattachment be achieved with this technique?” to “How well will the retina be reattached with this technique, and how well will the patient see?”
Maximizing the integrity of reattachment will naturally lead to improved functional outcomes, and this should be our primary goal as vitreoretinal surgeons.
There are a number of factors to consider when attempting to increase the integrity of reattachment. These factors range from choice of surgical technique, type and size of tamponade used, and patient positioning postoperatively. As mentioned above, PnR is associated with a greater chance of HIRA compared to PPV. Recent evidence also suggests that immediate face-down positioning after PPV (with log roll to face-down) with no intervening head elevated position also reduces the risk of LIRA. Finally, choice of tamponade can also influence this, as silicone oil likely causes less LIRA compared to gas because of the lower buoyant force applied to the retina with a smaller area of contact.
If one chooses to perform PPV with gas, in addition to log roll to face-down positioning, one may also consider converting PPV to an RPE pump-based procedure. In other words, the PPV can be carried out as usual; however, at the completion of surgery, air fluid exchange is avoided or minimized to end up with the smallest gas fill possible.
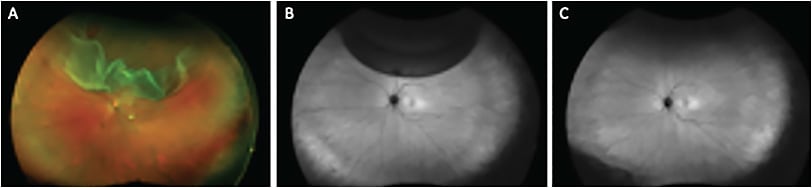
In minimal gas vitrectomy (MGV), air fluid exchange is completely avoided and a small expansile bubble of 0.6cc of pure SF6 gas is injected at the completion of surgery.3
The patient positions similar to how they would for PnR, and the retina reattaches naturally by the action of the RPE pump. This is likely to lead to a better integrity of reattachment compared with standard PPV with a full gas fill in terms of retinal displacement (LIRA/HIRA) (Figure 2).
In order to perform integrity-based surgery and maximize functional outcomes following retinal detachment repair, a vitreoretinal surgeon must truly be comfortable will all methods of retinal reattachment, including PnR, PPV, SB, and PPV-SB. Although most vitreoretinal surgical training programs offer substantial experience with PPV, many programs are lacking in terms of PnR.
In the next issue, I will describe my approach to PnR and how to maximize anatomic outcomes with this elegant office-based technique for routine and complex cases. NRP
REFERENCES
- Hillier RJ, Felfeli T, Berger AR, et al. The pneumatic retinopexy versus vitrectomy for the management of primary rhegmatogenous retinal detachment outcomes randomized trial (PIVOT). Ophthalmol. 2019;126(4):531-539.
- Brosh K, Francisconi CLM, Qian J, et al. Retinal displacement following pneumatic retinopexy vs pars plana vitrectomy for rhegmatogenous retinal detachment. JAMA Ophthalmol. 2020;138(6):652-659.
- Muni RH, Felfeli T, Figueiredo N, Marafon SB, Escaf LS, Juncal VR. Minimal gas vitrectomy technique for reducing risk of retinal displacement following rhegmatogenous retinal detachment repair. Retinal Cases Brief Rep. 2020. [online ahead of print]