







Segmental buckles provide localized support of the break without the need for 360°-encircling elements and can be an excellent option to repair rhegmatogenous retinal detachments. Their success rates are better than pneumatic retinopexy and similar to vitrectomy or 360° scleral buckling.1-4 They have the advantage of minimal to no refractive changes, no requirement of gas tamponade, no postoperative positioning, no progression of cataract, and minimal discomfort.5 A surgeon with training of primary buckles or encircling buckles with vitrectomy can easily transition to segmental buckling.
PREOPERATIVE EXAM
The most critical aspect when considering segmental buckling is the preoperative exam. Identification of breaks and other pathologies will help guide the decision process for the ideal candidate. A retinal detachment due to a single break or several breaks within 1 to 3 clock hours is a good candidate for segmental buckling. Lattice degeneration or atrophic holes in other quadrants of attached retina does not exclude the option of a segmental buckle. However, those areas should be treated with barrier laser/cryopexy preoperatively or at the time of the surgery.
TECHNIQUE
- Peritomy. When starting to perform segmental buckles, I recommend a 360° peritomy and isolating all 4 recti muscles (as one would do for a standard encircling buckle.) As a surgeon becomes more comfortable with segmental buckling and confident with identifying the pathology, they can transition to a limited peritomy in the quadrant of the breaks. Only 2 of the muscles need to be isolated and a bridle suture at the limbus can be placed 180° opposite from the peritomy. This will allow the same level of maneuverability as isolating 4 muscles. However, cosmetically, this is much nicer for the patient, as only 3 to 4 clock hours of conjunctiva has been disrupted. In addition, this saves ideal real estate if the patient ever develops other ocular pathologies, such as glaucoma, that would require surgery.
- Radial or circumferential. In segmental buckling, the buckle can be placed circumferentially or radially. The buckling element should provide at least 1 mm additional support beyond the width of the break. The width of the mattress sutures should be 1 mm to 2 mm wider than the width of the element.I recommend starting with a circumferential segmental buckle for surgeons who are transitioning into segmental buckling. Although the circumferential element can be placed for any number of clock hours, I typically prefer to place it in one whole quadrant. Typically, 2 horizontal mattress sutures are placed in the quadrant or a long figure-8 suture can be placed.6 If the ends of the segmental buckle are more than 4 mm away from the mattress sutures, single pass anchor sutures are recommended for the ends.
A radial element is even a more minimalistic approach. Ideally a sponge is placed radially in patients with a single break that is smaller than 1 clock hour or a group of breaks that are less than 1 clock hour. Vertical mattress sutures 1 mm to 2 mm wider than the width of the element should be placed in order to provide imbrication and ideal positioning. - Type of element. Sponges, such as a 510 (5 mm wide x 2.5 mm half round depth) or a 511 (7 mm wide with 2.5 mm half round depth), are very versatile. They provide excellent options for a circumferential or radial orientation. In addition, a sponge with a groove (506-G or 507-G) can be used for surgeons who want to transition into segmental buckling but prefer an encircling element to be added with their segment. If the sponge is placed circumferentially, it is also compatible with other radial elements, such as a 103 or 106, if additional posterior support is needed in specific areas.
ADVANTAGES
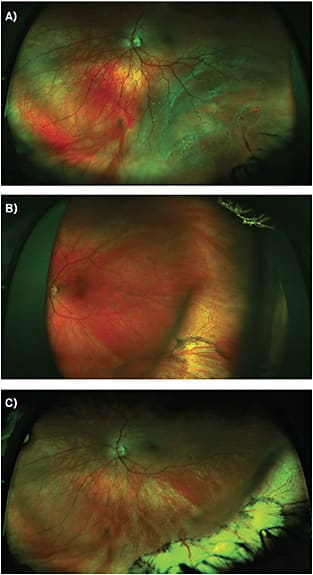
Segmental buckling provides similar success rates to traditional encircling buckling procedures, as well as pars plana vitrectomy. Changes in refractive error is minimal to none and significantly less than encircling elements. This can be particularly important for younger patients who are already myopic or underwent surgery, such as LASIK, to correct their refractive error (Figure 1). Postoperative pain also tends to be significantly less than traditional encircling surgeries as there is not as much manipulation of recti muscles nor imbrication of the globe 360°. The risk of long-term complications of encircling buckles, such as diplopia, congestion of the vortex veins, or macular choroidal ischemia, is also not present.7,8 Segmental buckles can also be done efficiently (typically in 45 minutes).
KEY CONSIDERATIONS
Adequate preoperative planning and confidence of having identified all pathology is the key to successful segmental buckling. One way to transition to segmental buckling is to do a segmental when planning to do a vitrectomy with buckle. Perform the buckle like a primary segmental buckle, which would include marking the break externally and placing sutures accordingly. Seeing the placement of the segmental during vitrectomy will give the confidence and comfort to the surgeon of adequate buckle technique. This can then allow you to transition to primary segmental buckles. I perform segmental buckles on phakic retinal detachments with breaks within 1 quadrant (3 clock hours of each other) and no other breaks involving the detachment in other quadrants. Patients who are concerned for refractive error and are better candidates for buckling also benefit from segmental buckles (post-LASIK, high myopes, multifocal IOLs). Segmental buckles should be within the tool set of vitreoretinal surgeons when repairing retinal detachments. NRP
REFERENCES:
- Kreissig I, Rose D, Jost B. Minimized surgery for retinal detachments with segmental buckling and nondrainage. An 11-year follow-up. Retina. 1992;12(3):224-231.
- Paulus Y, Leung LS, Pilyugina S, Blumenkranz MS. Comparison of pneumatic retinopexy and scleral buckle for primary rhegmatogenous retinal detachment repair. Ophthalmic Surg Lasers Imaging Retina. 2017;48(11):887-893.
- Wickham L, Connor M, Aylward GW. Vitrectomy and gas for inferior break retinal detachments: are the results comparable to vitrectomy, gas, and scleral buckle? Br J Ophthalmol. 2004;88(11):1376-1379.
- Weichel ED, Martidis A, Fineman MS, et al. Pars plana vitrectomy versus combined pars plana vitrectomy-scleral buckle for primary repair of pseudophakic retinal detachment. Ophthalmology. 2006;113(11):2033-2040.
- Smiddy WE, Loupe DN, Michels RG, Enger C, Glaser BM, deBustros S. Refractive changes after scleral buckling surgery. Arch Ophthalmol. 1989;107(10):1469-1477.
- Min H Y, Chen D, Chen Y, Dong F T. One “8”- shaped scleral suture to treat rhegmatogenous retinal detachment: a refined procedure of minimal scleral buckling. Genet Mol Res. 2014; 13(3):6665-6671.
- Iwase T, Kobayashi M, Yamamoto K, Yanagida K, Ra E, Terasaki H. Change in choroidal blood flow and choroidal morphology due to segmental scleral buckling in eyes with rhegmatogenous retinal detachment. Sci Rep. 2017;7:5997.
- Yoshida A, Feke GT, Green GJ, et al. Retinal circulatory changes after scleral buckling procedure. Am J Ophthalmol. 1983;95(2):182-188.